Let’s talk Cholesterol
Cholesterol is often viewed as something harmful, but the truth is more complex. It is a waxy, fat-like substance that plays a vital role in keeping your body healthy. Every cell in your body contains cholesterol, and it is essential for producing hormones, vitamin D, and substances that help digest food.
While cholesterol is necessary for normal body function, having too much of certain types can increase the risk of heart disease and stroke.
What Is Cholesterol?
Cholesterol is a type of lipid (fat) that circulates in your bloodstream. Your body naturally produces most of the cholesterol it needs in the liver. The rest comes from the foods you eat, particularly those high in saturated and trans fats.
Types of Cholesterol
Low-Density Lipoprotein (LDL) – "Bad" Cholesterol
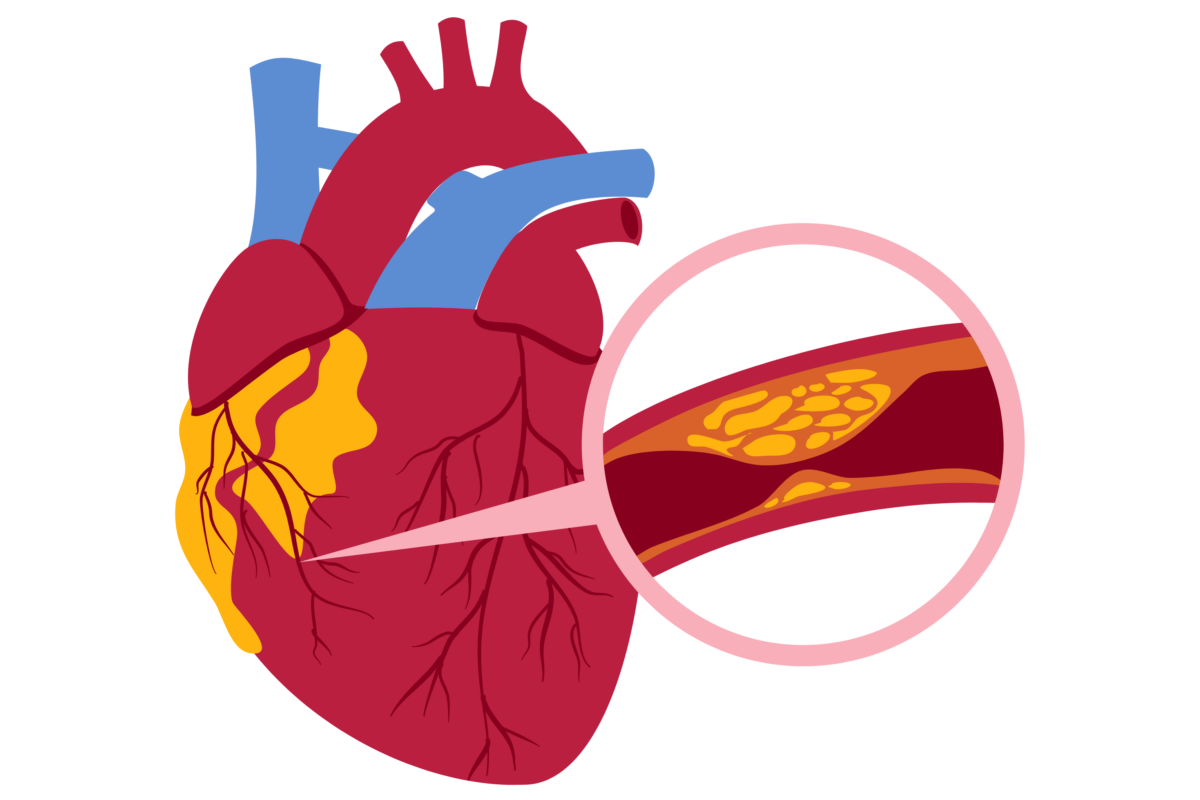
LDL cholesterol is often referred to as "bad cholesterol" because high levels can lead to the buildup of fatty deposits, known as plaque, inside your arteries. Over time, plaque narrows the arteries, making it harder for blood to flow. This condition, called atherosclerosis, increases the risk of:
Heart attack
Stroke
Peripheral artery disease
Lowering LDL cholesterol is a key goal in reducing cardiovascular risk.
High-Density Lipoprotein (HDL) – "Good" Cholesterol
HDL cholesterol is known as "good cholesterol" because it helps remove excess cholesterol from the bloodstream and carries it back to the liver, where it can be broken down and eliminated from the body.
Higher HDL levels are generally associated with a lower risk of heart disease.
Triglycerides
Although not a type of cholesterol, triglycerides are another important blood fat. High triglyceride levels, especially when combined with high LDL or low HDL, can further increase the risk of cardiovascular disease.
Why High Cholesterol Is a Concern
High cholesterol usually develops without causing noticeable symptoms. Many people are unaware they have elevated cholesterol until it is detected through a routine blood test.
If left untreated, high cholesterol can contribute to:
Coronary artery disease
Heart attack
Stroke
Reduced blood flow to the limbs
Because it is often symptom-free, high cholesterol is sometimes called a "silent risk factor."
Risk Factors for High Cholesterol
Several factors can increase cholesterol levels, including:
Diet high in saturated and trans fats
Lack of physical activity
Being overweight or obese
Smoking
Excessive alcohol consumption
Diabetes
Chronic kidney disease
Family history of high cholesterol
Increasing age
Some people inherit a genetic condition called familial hypercholesterolemia, which causes very high cholesterol levels even with a healthy lifestyle.
How Is Cholesterol Measured?
A lipid profile is a blood test used to measure cholesterol levels. It typically includes:
Total cholesterol
LDL cholesterol
HDL cholesterol
Triglycerides
How to Maintain Healthy Cholesterol Levels
Healthy lifestyle habits are the foundation of cholesterol management.
Eat a Heart-Healthy Diet
Focus on:
Fruits and vegetables
Whole grains
Beans and legumes
Nuts and seeds
Fish rich in omega-3 fatty acids
Healthy fats such as olive oil and avocado
Limit:
Fried foods
Processed meats
Sugary foods and beverages
Foods high in saturated and trans fats
Stay Physically Active
Aim for at least 150 minutes of moderate-intensity aerobic exercise each week. Activities such as brisk walking, cycling, swimming, or dancing can help improve cholesterol levels and support heart health.
Maintain a Healthy Weight
Even modest weight loss can improve cholesterol levels and reduce cardiovascular risk.
Avoid Smoking
Quitting smoking can improve HDL cholesterol and significantly lower the risk of heart disease.
Limit Alcohol Intake
Excessive alcohol consumption may increase triglyceride levels. Drinking in moderation, if at all, is recommended.
When Are Medications Needed?
Lifestyle changes alone may not be enough for everyone. Cholesterol lowering medications may be recommended if:
LDL cholesterol remains high despite lifestyle changes.
You have diabetes.
You have established heart disease.
Your calculated cardiovascular risk is high.
You have inherited high cholesterol.
Can High Cholesterol Be Prevented?
In many cases, yes. A balanced diet, regular exercise, maintaining a healthy weight, avoiding tobacco, and having regular health checkups can help prevent or delay the development of high cholesterol.
For individuals with inherited cholesterol disorders, early diagnosis and treatment are especially important.
*Disclaimer: This article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Consult your healthcare provider for personalized recommendations regarding cholesterol testing and management.
Visit us at oasisrockmedical.com/schedule to schedule a primary care preventive visit and get your cholesterol checked or call us at 6828826060 to make an appointment.


